A stent is an endoprothesis used to keep a cavity or vessel of the human body open. It is generally a cylindrical metal structure that can come in various sizes, diameters, structures and materials depending on the intended application.


A stent is an endoprothesis used to keep a cavity or vessel of the human body open. It is generally a cylindrical metal structure that can come in various sizes, diameters, structures and materials depending on the intended application.

Covidien – Medtronic balloon stent
A stent is inserted by catheterization using two main methods:
The stent is dilated by the catheter balloon: the stent is placed during an angioplasty, under local anesthesia. The probe is brought to the blocked artery where a small balloon is inflated at the narrowed area to crush the atheromatous plaques against the arterial walls. The stent is then inserted in order to keep the artery open once the balloon has been removed.
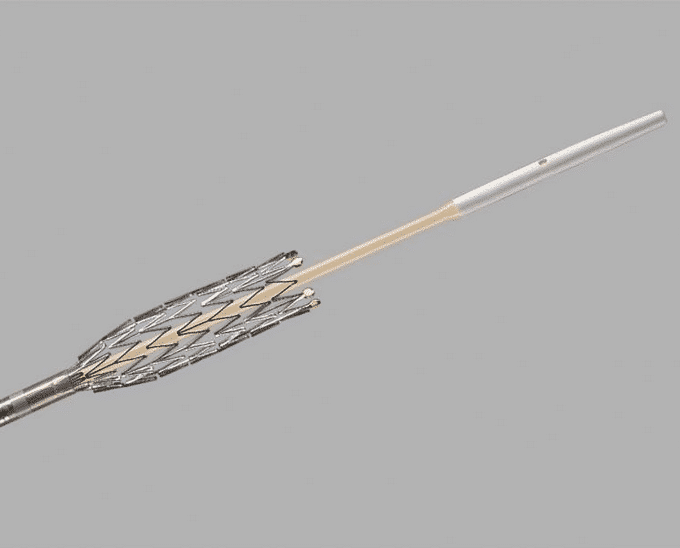
A COOK Medical self-expanding stent
Self-expanding stent: the stent isn’t set on a balloon but is instead compressed in a thin sheath. Once it’s been placed inside the artery of the occlusion site, the sheath is removed; the stent then expands and moves the intima of the artery outwards. It keeps the artery open by attaching itself to the walls.
Stents are mainly made from the following five types of materials: metallic, coated, drug eluting, bioresorbable and radioactive.

A Rontis Medical drug eluting coronary stent
Drug eluting stents are primarily used to reduce the risk of restenosis. They are composed of three elements: the metallic stent, the active drug and its delivery system, which is most often made of polymer.
The drug slowly being released is generally mainly sirolimus or paclitaxel. Both drugs have obtained the European CE conformity marking on the basis of evidence acquired in randomized trials.
The purpose of these antimitotic and/or anti-inflammatory agents deposited on the stent is to block intimal proliferation in situ. Since they have been created, drug-eluting stents have significantly reduced restenosis, which is particularly common in angioplasty and bare stent implantation
The main risks associated with inserting stents are restenosis, clotting, kidney risks and vessel rupture.
Several parameters can be used to limit the risk of the restenosis associated with inserting a stent. The first, as we have seen, is the use of drug-eluting stents to contain intimal proliferation.
But that’s not the only parameter. The dimensions of the stent, i. e. its length and width, as well as the mesh size of the stent graft are also important. Technological developments over the past twenty years have led to many advances. In the past, the slotted tubes used were inflexible and caused major problems during implantation. The so-called “coil” stents had insufficient radial strength, which could lead to tissue prolapse.
Today, the physical parameters of stents have greatly improved, including better stent release, new mesh size for better support and better visibility during radiographic examinations. These improvements have had a significant impact on procedural success and restenosis rates.


 (1 votes, average: 5.00 out of 5)
(1 votes, average: 5.00 out of 5)